“Digital chiropractic marketing
agencies promise the world.
We give you something REAL:
your territory.”
Lock In Your ZIP Code For Just $997/Month, Cancel Anytime.

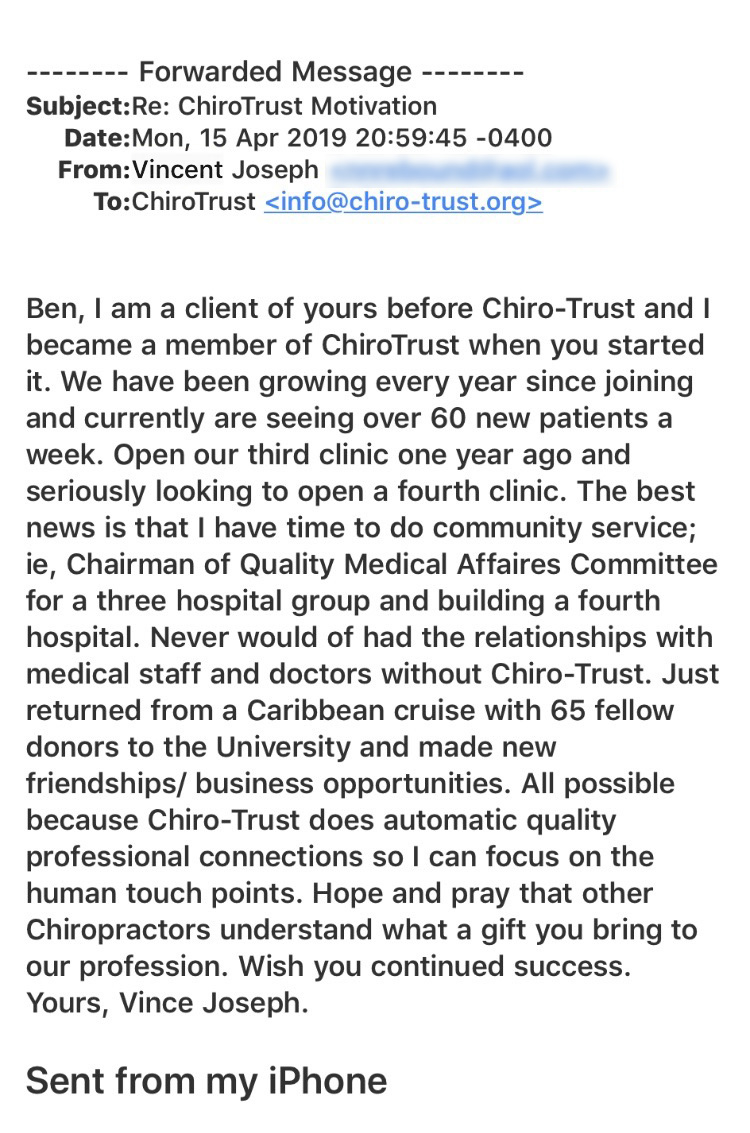
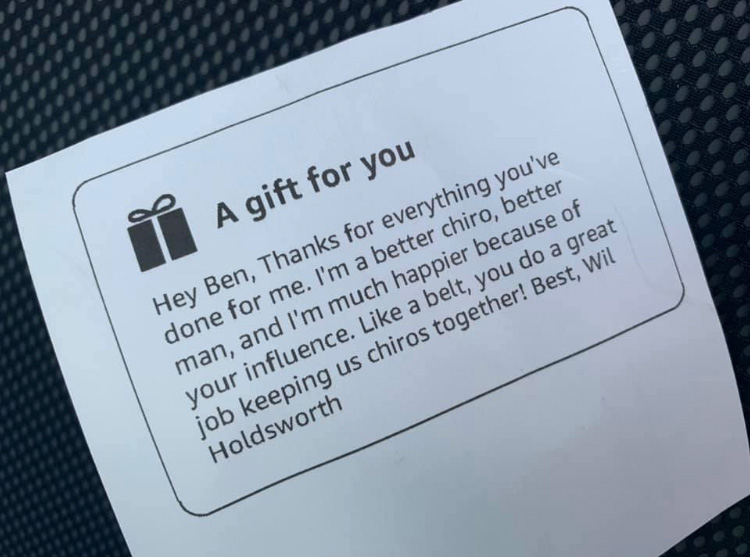
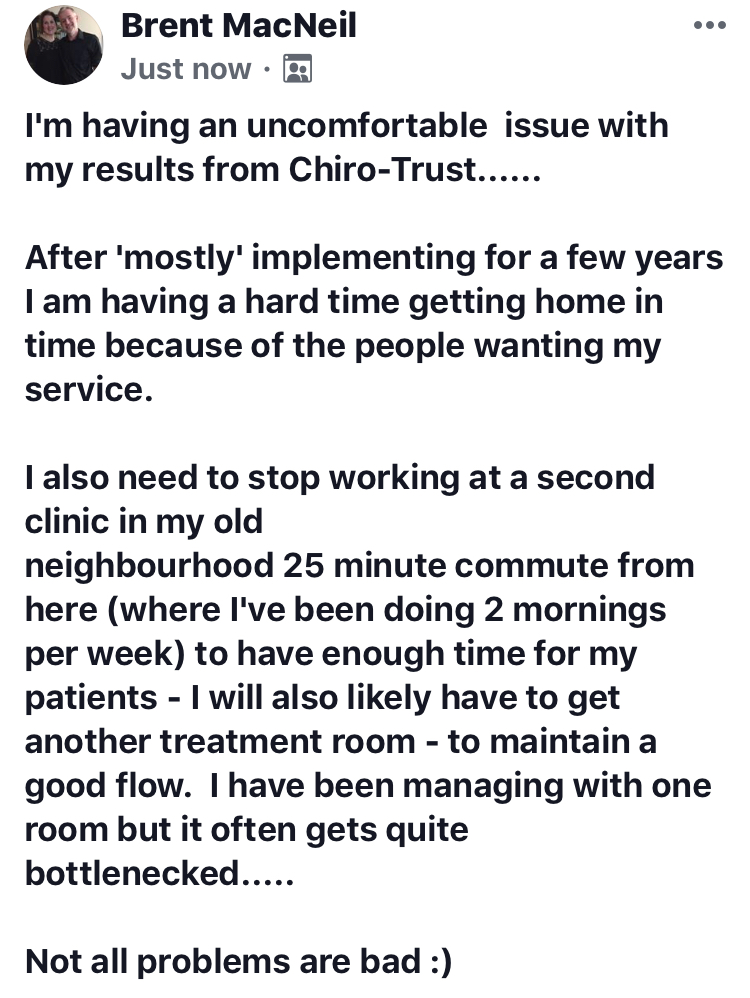
ChiroTrust turns your community and past patients into a predictable flow of appointments by educating, reminding, and re-engaging your town and patients every single day—done for you, under your name—so your ZIP code becomes your #1 source of new patients and repeat visits.
WHAT YOU GET
- Instant local authority.
Your name goes on expert-written, educational content going out to your community and patient list every single day, so you become the chiropractor they think of first. - No tech. No staff. No extra hours.
If you can focus on your patients, we’ll quietly make you the go-to chiropractor in your ZIP code. - Built by chiropractors, for chiropractors.
We’ve already burned money on the stuff that doesn’t work. You just plug into what does.
WHY THIS IS DIFFERENT FROM A “DIGITAL CHIROPRACTIC MARKETING AGENCY”
- ZIP code exclusivity.
Only one chiropractor per ZIP. If you don’t claim it, we’ll quietly give it to a competitor. - Daily Facebook “Always On” marketing—paid by us.
We run and fund a steady, educational presence on Facebook for your community. You’re not gambling on ad spend or learning Ads Manager. - A proven daily referral and return-visit system.
Short, value-based “staying in touch” messages that keep past patients engaged, referring, and coming back in—without begging or discounting. - Your own Online Information Center.
A branded, content-rich “Online Information Center” that positions you as the local health authority and funnels interested visitors into your practice.
THE OFFER
- Month-to-month at $997—cancel anytime.
No contracts. No setup fees. No long-term commitments. - Grandfathered pricing.
As long as you keep your ZIP code, your rate never goes up, even as new doctors pay more.